Primary Hyperaldosteronism: An Unusual but not a Rare Entity
Article Sidebar
Main Article Content
Abstract
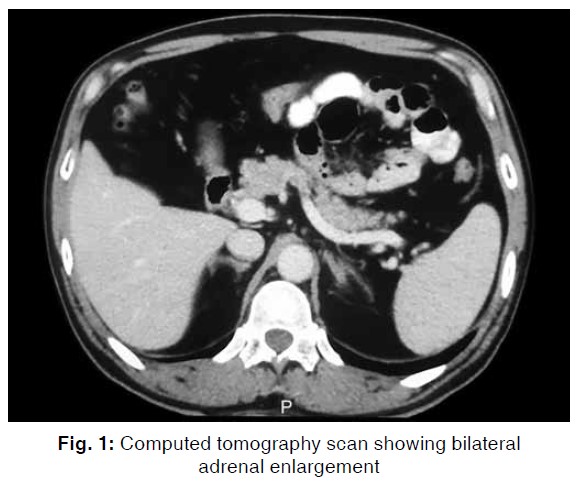
A 36 years old gentleman presented to hospital with symptoms of viral illness. In addition to fever, he was found to have blood pressure of 240/160 mm Hg which was confirmed by repeated measurements. There was no evidence of target organ damage. His febrile illness turned out to be due to swine flu. Due to severe hypertension, he was admitted to the intensive care unit (ICU) for parenteral antihypertensive drug therapy. He had unexplained severe hypokalemia and metabolic alkalosis. The possibility of primary hyperaldosteronism was considered, plasma aldosterone level was high and plasma renin activity was low, confirming the (biochemical) diagnosis of hyperaldosteronism. He underwent additional work-up and was given specific antihypertensive drugs. The case illustrates classical features of primary hyperaldosteronism, diagnostic and therapeutic considerations.
Metrics
Article Details

This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.
All open access articles published in the journal are distributed under the terms of the CC-BY-NC-SA 4.0 license (Creative Commons Attribution-Non-commercial 4.0 International License) which permits unrestricted use, distribution, and reproduction in any medium, for non-commercial purposes, provided the original work is properly cited. Under Creative Commons, authors retain copyright in their articles.
References
Ram CVS. Primary aldosteronism—recognition and management. Rhode Island Med J 1977;60(6):301-305.
Ram CVS. Primary aldosteronism—its role in hypertension. Consultant 1981;21:2-11.
Ram CVS. Hypertension: when to suspect underlying pheochromocytoma or aldosteronism? Consultant 1996;33: 147-153.
Lim PO, Rodgers P, Cardale K, et al. Potentially high prevalence of primary aldosteronism in a primary-care population. Lancet 1999 Jan 2;353(9146):40.
Loh KC, Koay ES, Khaw MC, et al. Prevalence of primary aldosteronism among Asian hypertensive patients in Singapore. J Clin Endocrinol Metab 2000;85(8):2854-2859.
Stowasser M, Gordon RD. The aldosterone-renin ratio for screening for primary aldosteronism. Endocrinologist 2004;14:267-276.
Stowasser M, Gordon RD. Primary aldosteronism: careful investigation is essential and rewarding. Mol Cell Endocrinol 2004;217(1-2):33-39.
Oliveri O, Ciacciarelli A, Signorelli D, et al. Aldosterone to renin ratio in a primary care setting: the Bussolengo study. J Clin Endocrinol Metabol 2004;89(9):4221-4226.
Rutherford JC, Taylor WL, Stowasser M, et al. Success of surgery in primary aldosteronism judged by residual autonomous aldosterone production. World J Surg 1998;22(12):1243-1245.
Rutherford JC, Stowasser M, Tunny TJ, et al. Laparoscopic adrenalectomy. World J Surg 1996;20(7):758-760.
Parthasarathy HK, Ménard J, White WB, et al. A double-blind, randomized study comparing the antihypertensive effect of eplerenone and spironolactone in patients with hypertension and evidence of primary aldosteronism. J Hypertens 2011;29(5):980-990.
Stowasser M, Gordon RD, Rutherford JC, et al. Diagnosis and management of primary aldosteronism. J Renin Angiotensin Aldosterone Syst 2001;2(3):156-169.
Rossi GP, Sacchetto A, Visentin P, et al. Changes in left ventricular anatomy and function in hypertension and primary aldosteronism. Hypertens 1996;27(5):1039-1045.
Rossi GP, Bernini G, Desideri G, et al. Renal damage in primary aldosteronism: results of the PAPY study. Hypertens 2006;48(2):232-238.