
Evaluation of Anterior Segment Parameters by using Pentacam and Gonioscopy after Prophylactic Laser Peripheral Iridotomy among primary angle close suspect
Article Sidebar
Main Article Content
Abstract
Aim: To evaluate laser Perifheral iridotomy (LPI) changes on anterior segment parameters (ASP) among primary angle closure suspect (PACS) using the Pentacam and gonioscopy.
Methods: This comparative, prospective, Interventional Study was conducted between August 2019 to May 2021. 100 eyes of 100 PACS were included. Anterior chamber angle (ACA), central anterior chamber depth (ACD), anterior chamber volume (ACV) and central corneal thickness (CCT) were recorded from the Pentacam before and one month after LPI. ACA was graded according to Shaffer classification using the Goldmann gonioscopy. The paired samples t-test was used to compare the difference in ASP while Wilcoxson signed-rank test was used to assess the ACA grading.
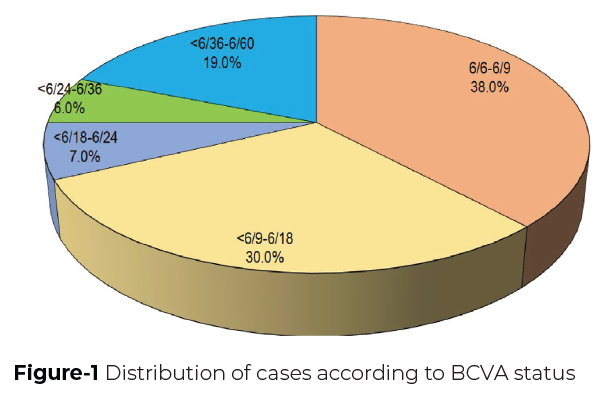
Results: Among enrolled males were 41% & mean age was 50.56 ± 6.03 SD (ranged 40 to 60 years). 27% had previous glaucoma treatment history and 88% had positive family history of glaucoma. Mild lenticular sclerosis was present in 49%. Maximum number of cases had BCVA in > 6/18 (68%). Pentacam evaluation pre-intervention found mean ACA, ACD, ACV and CCT were 26.73 ± 1.05º, 2.09 ± 0.12 mm, 78.51 ± 7.12 mm3 and 510 ± 6.5 μm, respectively. Following LPI mean ACA, ACD and ACV showed an increase of 1.47±0.72º, 0.08±0.07 mm, and 51.08±20.56 mm3, respectively. Statistically, these changes were significant (p<0.001) except for central corneal thickness (p=0.454). Gonioscopic evaluation pre and post-LPI reveal that the angle width increased significantly in all quadrants (P<0.001) except inferior quadrant (P=0.025).
Conclusion: Both Gonioscopy and Pentacam can easily access efficacy of LPI. Pentacam is more sensitive to minor changes.
Article Details

This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.
Under Creative Commons the Authors retain ownership of the copyright for their content. The authors assign exclusive commercial re-use rights of the article to the Journal.
All open access articles published are distributed under the terms of the CC BY-NC 4.0 license (Creative Commons Attribution-Non-Commercial 4.0 International Public License as currently displayed at http://creativecommons.org/licenses/by-nc/4.0/legalcode) which permits unrestricted use, distribution, and reproduction in any medium, for non-commercial purposes, provided the original work is properly cited.
Authors agree to the open access publication policy of the Journal.
References
Chaurasia RK, Kapil V, YasirZHCorrelation Of Visual Acuity With Macular Thickness In Early And Advanced Stages Of Primary Open Angle Glaucoma.DJO 2021;31:37-42.
Quigley HA. Number of people with glaucoma worldwide. Br J Ophthalmol. 1996; 80(5):389–93.
Cyrlin M.N. (2014) Primary and Secondary Angle-Closure Glaucomas. In: Samples J., Schacknow P. (eds) Clinical Glaucoma Care. Springer, New York, NY.
Foster PJ, Buhrmann R, Quigley HA, Johnson GJ. The definition and classification of glaucoma in prevalence surveys. Br J Ophthalmol. 2002; 86(2):238–42.
Prum BE, Herndon LW, Moroi SE, et al. Primary Angle Closure Preferred Practice Pattern(®) Guidelines. Ophthalmology. 2016; 123(1):P1–40.
Thomas R, Parikh R, Muliyil J, Kumar RS. Five-year risk of progression of primary angle closure to primary angle closure glaucoma: A population-based study. Acta Ophthalmol Scand. 2003; 81(5):480–5.
Mingguang He, David S. Friedman, Jian Ge et al. Laser Peripheral Iridotomy in Primary Angle-Closure Suspects: Biometric and Gonioscopic Outcomes. Ophthalmology 2007; 494–500.
Dabasia PL, Edgar DF, Murdoch IE, Lawrenson JG. Noncontact Screening Methods for the Detection of Narrow Anterior Chamber Angles. Invest Ophthalmol Vis Sci. 2015;56(6):3929-35.
Shinoj VK, Hong XJJ, Murukeshan VM, Baskaran M, Aung T. Progress in Anterior Chamber Angle Imaging for Glaucoma Risk Prediction—A Review on Clinical Equipment, Practice and Research. Med. Eng. Phys. 2016;38:1383–1391
Bevara A, Banigallapati S, Medikonda M, Potti S. Pentacam Based Quantification of the Changes in Anterior Chamber Morphology Following Laser Peripheral Iridotomy in Primary Angle Closure Suspects – A Novel Approach. DJO 2020; 30: 51-56.
Esmaeili A, Barazandeh B, Ahmadi S, et al. Assessment of the anterior chamber parameters after laser iridotomy in primary angle close suspect using Pentacam and gonioscopy. Int J Ophthalmol. 2013;6(5):680-4.
Kaur P, Gusain P, Singh J, Mahajan. Evaluation of the anterior chamber parameters after laser iridotomy in primary angle closure suspect: pentacam and gonioscopy study. Global Journal For Research Analysis. 2019; 8(1): 14-16.
Charan J, Biswas T. How to Calculate Sample Size for Different Study Designs in Medical Research? Indian J Psychol Med. 2013; 35(2): 121–126.
Xiaoyu Li, Zheng Wang, Qun Cao, et al. Pentacam could be a useful tool for evaluating and qualifying the anterior chamber morphology. Int J Clin Exp Med 2014; 7(7): 1878-1882.
Zebardast N, Kavitha S, Krishnamurthy P, et al. Changes in Anterior Segment Morphology and Predictors of Angle Widening after Laser Iridotomy in South Indian Eyes. Ophthalmology. 2016;123(12):2519-2526.
Jain R, Grewal D, Grewal SPS. Quantitative Analysis of Anterior Chamber following Peripheral Laser Iridotomy using Pentacam in Eyes with Primary Angle Closure. 2013;23(1):55-60.
Vajaranant TS, Nayak S, Wilensky JT, Joslin CE. Gender and glaucoma: what we know and what we need to know. Curr Opin Ophthalmol. 2010;21(2):91-99.
O'Brien JM, Salowe RJ, Fertig R, et al. Family history in the primary open-angle African American glaucoma genetics study cohort. American journal of ophthalmology. 2018 1;192:239-47.
Saxby E, Cheng K, O’Connell N, Sanders R, Agarwal PK. Is there an association of socioeconomic deprivation with acute primary angle closure?. Eye. 2021;11:1-7.
Chong Seong NT, Yaakub A, Jalil RA, et al. Effect of physical activity on severity of primary angle closure glaucoma. Therapeutic advances in ophthalmology. 2019;11:2515841419864855.